Gastric Dieulafoy Lesion
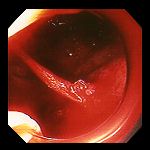
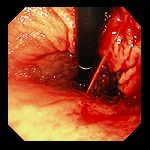

Left: Massive pulsatile bleeding in the gastric fundus of a 48 year-old man who presented with melena and hemorrhagic shock. Narrowed view through the banding apparatus attached to the tip of the endoscope. There was no ulcer surrounding the point of bleeding. Center & Right: 74 year-old woman who presented with acute hematemesis (vomiting blood). Exam revealed pulsatile bleeding just below the esophagogastric junction, seen on retroflexion (note that we are looking back on the instrument as it enters the stomach from the esophagus). The jet of blood was emanating from a tiny defect in the mucosa, with no associated visible ulceration. The bleeding responded well to heater-probe cauterization, and did not recur.

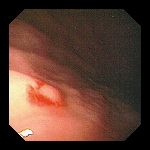
Left: 70 year-old woman who also presented with acute hematemesis (vomiting blood). Endoscopy demonstrated a nonpulsatile but continuous flow of blood from a focus in the proximal gastric body, seen on retroflexion. Right: The site was repeatedly washed with cold water, and the bleeding briefly stopped, revealing this underlying protruding vessel with no visible ulcer. The lesion was cauterized and there was no further bleeding.


Left: 72 year-old an with hematemesis. At endoscopy an intermittent pulsatile stream of blood was identified, with no underlying lesion visible between bleeding spurts. Right: The site was banded, successfully controlling the bleeding. The mucosal bleb created by banding is visible through the translucent endoscope attachment used in the banding process.

Bleeding vessel in a 53 year-old woman who presented with hematemesis. Bleeding was controlled by the application of metallic hemostatic clips.
Endoscopic images Copyright © Atlanta South Gastroenterology, P.C. All rights reserved.
Logo is Registered Trademark ® of Atlanta South Gastroenterology, P.C.
This site is presented for educational and general informational purposes only. It does not purport to offer medical advice for any specific medical condition or individual patient. We regret that we cannot provide individualized medical advice online, either via this web site or via email. Please refer to our "Notable Web Sites" section, which offers links to several excellent online sources of additional medical information.